
The Acid Test Has Changed: What the New Deprivation of Liberty Ruling Means for Practice
Date: 3rd June, 2026.
Authored By: Doris Sheridan | doris@sheridanconsult.co.uk
There is a kind of legal change that arrives with clear operational instructions in a new form, a revised threshold, a date from which things work differently. And then there is the kind that arrives as a shift in principle, one that will take time, professional honesty, and careful thought to absorb and translate into practice.

The Supreme Court's judgment handed down on 2nd June 2026, in UKSC/2025/0042, is the second kind. And for everyone working in DoLS, Best Interests Assessment, or mental capacity practice, I think it deserves a moment of serious attention before we reach for the updated guidance documents.
What the Court has decided, and why it matters
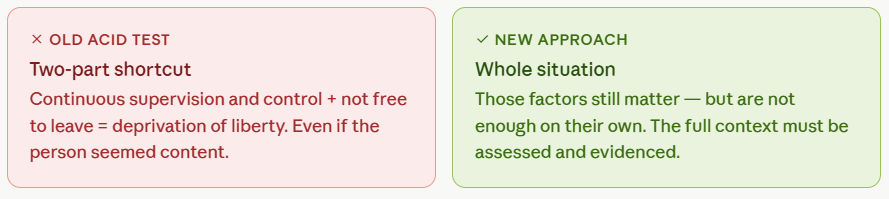
For over a decade, the acid test derived from the 2014 Cheshire West ruling has shaped how health and social care professionals approach the question of deprivation of liberty. The practical shortcut was clear: if a person was under continuous supervision and control, and was not free to leave, that amounted to a deprivation of liberty under Article 5 of the European Convention on Human Rights regardless of how settled they appeared, regardless of how thoughtfully their care had been arranged.
The Supreme Court has now overruled that test. It has said, plainly, that Cheshire West went too far.
Those two factors supervision, control, and restriction of movement remain relevant considerations. But they are no longer sufficient on their own. What the Court has established is that valid consent under Article 5 is an autonomous legal concept, distinct from the question of capacity under domestic mental capacity law. A person may lack capacity to make decisions about their care and treatment under the Mental Capacity Act, and yet still be capable, in Article 5 terms, of communicating whether they are happy or unhappy with their living arrangements and that communication can amount to valid consent.
The implication is significant: lack of MCA capacity no longer automatically equals lack of Article 5 consent.
The two areas I am most concerned about
I want to be direct here, because I think this ruling will be misread in two directions and both carry risk for the people we support.
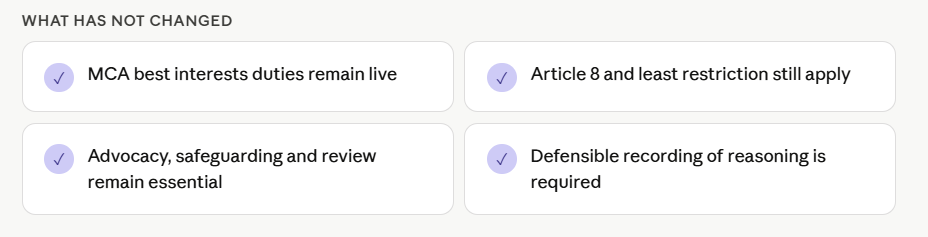
The first is the conclusion that safeguards no longer matter. They do. Article 8 rights, best interests duties under the MCA, the obligation to use the least restrictive option, advocacy, care planning, safeguarding enquiries, and the duty to review do not disappear because Article 5 may not be engaged in a particular case. If anything, this judgment places greater demands on practitioners not fewer.
The second area is more subtle, and in some ways more troubling: treating apparent contentment as consent. The Court was explicit on this point. Silence is not consent. Passivity is not consent. The absence of objection is not consent. What is required is something more active genuine evidence that the person, in their own way and through their own communication, is expressing a positive acceptance of their situation.
That distinction matters enormously in practice. Many of the people we work with have learned, over years of institutional care, not to object. Some have experienced consequences for doing so. Some lack the communication tools to make resistance visible. Some present as settled and cooperative in ways that are, in truth, responses to environments where alternatives have never been meaningfully offered. Practitioners will need to be alert to all this actively, not passively reassured.
What Assessment now requires
The judgment moves practice away from a two-part checklist and towards something more demanding: a genuine analysis of the person's whole situation.
That means asking what kind of restrictions are in place: the nature, the purpose, how long they have been in operation, and how they are being implemented day to day. It means asking whether the arrangements, looked at honestly, resemble ordinary care and support, or whether they carry the character of detention. It means considering whether there is any element of coercion: force, locked exits, isolation, restricted contact, or fear that the person may not be able to communicate directly.
It means assessing and evidencing the person and situation properly. Not a single visit or a single conversation, but a sustained effort to understand how they communicate, what they value, what they return to willingly, and what they avoid or resist. Family and staff knowledge matters here. So do records of the small, everyday signals the choices someone makes, the places they ask to go, the people they reach for. These things, taken together, are what genuine consent looks like. They are also what a defensible record of that consent requires.

And it means being honest in our recording. A record of reasoning in this new landscape should clearly set out what was observed, what the person communicated and how, what restrictions exist and why, what alternatives were genuinely considered, and on what basis the practitioner has concluded whether the Article 5 threshold is or is not met. That level of transparency is not administrative burden it is professional integrity.
What has not changed
It is worth saying this clearly, because I think the temptation in the wake of any significant legal shift is to assume that less is now required.
Even where Article 5 is not engaged, the full framework of protection under the Mental Capacity Act remains live. Best interests’ decision-making, the least restriction principle, the duty to review, and the right to advocacy do not depend on a deprivation of liberty being established. The people we support deserve that standard of practice regardless of whether a formal authorisation is in place.
What this asks of us as Practitioners
For England and Wales, statutory processes and local operational guidance will need time to develop in light of this ruling. That is realistic and right implementation will require careful translation rather than reactive change. In the meantime, the professional obligation remains what it has always been: thoughtful, honest, well-reasoned practice that holds the person at its centre and records its thinking clearly enough to withstand scrutiny.
What this judgment changes is the framework. What it does not change and should never change is the commitment to treating each person as an individual whose situation deserves to be understood, not categorised.
That has always been the standard this work calls for. The law has now made it explicit.
If this is raising questions in your own professional context about practice, about team readiness, or about how to translate this change into defensible day-to-day decision-making I would welcome the conversation.