
ISO 9001:2015 What It Actually Demands, and Why It Matters in Health and Social Care
Date: 8th May 2026
Authored By: James Sheridan | james@sheridanconsult.co.uk
Achieving ISO 9001 certification is a significant milestone. But understanding what the standard truly demands is what separates organisations that hold it from organisations that are transformed by it.
That is the lens through which I want to share these reflections. Having recently completed my ISO 9001:2015 Lead Auditor training, I want to share what I have taken away from working through the standard in depth not as a theoretical overview, but as a practical reflection on what it demands from health and social care organisations operating in a regulated, high-scrutiny environment.

1. What ISO 9001:2015 Actually Is
ISO 9001 is the internationally recognised standard for Quality Management Systems (QMS). Over one million organisations hold certification globally. In the UK alone, more than 30,000 businesses are certified and that number includes NHS suppliers, local authority contractors, and independent care providers.
The current version, ISO 9001:2015, introduced risk-based thinking as a core requirement. It moved away from prescriptive processes and toward a framework that asks organisations to understand their context, identify what could go wrong, and build systems that prevent failure rather than simply respond to it.
The structure runs across 10 clauses. Clauses 1 to 3 are contextual. Clauses 4 to 10 are where the real work is and where most organisations either build something genuinely functional or fall short.
A revised version is expected in 2026, with greater emphasis on sustainability, climate risk, and digital transformation. Organisations that understand the current standard well will be far better positioned to adapt.
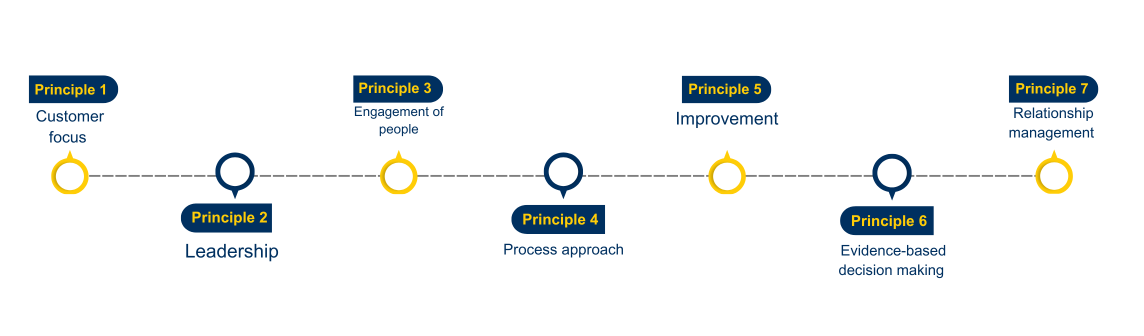
The 7 Principles: And What They Mean in Practice
Seven quality management principles underpin ISO 9001. These are not aspirational values. They are the operating logic of the entire standard.
Customer focus sits first for a reason. In health and social care, the "customer" is the person receiving care. Every process, every decision, every audit should ultimately trace back to whether it improves outcomes for that person. Collecting feedback, acting on complaints, and aligning performance indicators with service user experience are all direct expressions of this principle.
Leadership is about more than having a named director on a quality policy. ISO 9001 expects visible, accountable leadership that drives quality from the top, not delegates it to a compliance manager and moves on. In organisations I work with, this is often where the gap is widest.
Engagement of people means that staff at every level understand the organisation's quality objectives and feel empowered to contribute to them. A care worker who can identify a risk and knows exactly what to do with that information is living this principle. One who has never seen the quality policy is not.
Process approach is about consistency. Not every outcome can be controlled, but every process can be designed. Mapping how work actually gets done, not how it is supposed to get done on paper, is where quality improvement begins.
Improvement is ongoing, not periodic. ISO 9001 requires a functioning system for identifying nonconformities, completing corrective actions, and tracking whether those actions have worked. In a CQC context, this maps directly onto the well-led domain.
Evidence-based decision-making is non-negotiable. Decisions about staffing, risk, care planning, and resource allocation must be grounded in data. Gut feeling is not a quality management system.
Relationship management extends to commissioners, suppliers, partners, and regulators. In health and social care, this includes ICBs, local authorities, and inspection bodies. Managing those relationships proactively, rather than reactively, strengthens every other part of the system.
The 10 Clauses: A Practitioner's Summary
Clauses 4 to 10 form the operational backbone of the QMS. Here is what each one demands in plain terms:
Clause 1: Scope: This clause defines the boundaries of the standard what it covers and what it applies to. For health and social care organisations, this means being clear about which services, sites, and functions fall within the QMS. A vague or poorly defined scope creates gaps that show up immediately under audit. Clarity here sets the foundation for everything that follows.
Clause 2: Normative References: This clause references ISO 9000:2015 the companion standard that provides the vocabulary and foundational concepts underpinning ISO 9001. It is not a requirement to implement separately, but understanding the terminology it defines matters. Auditors and assessors use this language precisely. Organisations that do not speak it fluently often struggle to evidence compliance clearly.
Clause 3: Terms and Definitions: Directly linked to Clause 2, this clause establishes the shared language of the standard. In health and social care, where terminology already varies significantly between the NHS, local authorities, and independent providers, having a consistent internal vocabulary aligned to ISO 9000 reduces miscommunication and strengthens documentation quality across the board.
Clause 4: Context of the Organisation: Know your environment. Understand who your stakeholders are, what they expect, and what internal and external factors affect your ability to deliver quality. For health and social care providers, this includes commissioners, regulators, workforce pressures, and the needs of the people you support.
Clause 5: Leadership: Senior management must be directly involved in the QMS not just signatories on a policy. Quality objectives must be set at leadership level and communicated across the organisation.
Clause 6: Planning: Risk must be identified and managed proactively. Quality objectives must be measurable and integrated into operational planning not treated as separate from day-to-day delivery.
Clause 7: Support: Resources, training, infrastructure, and communication systems must support the QMS. If staff are not competent, aware of quality objectives, and equipped to do their jobs, the system fails regardless of what the documentation says.
Clause 8: Operation: This is where care is actually delivered. Processes must be defined, controlled, and traceable. Outsourced functions such as agency staffing or specialist services must be managed to the same standard.
Clause 9: Performance Evaluation: Internal audits, KPI monitoring, customer feedback, and management reviews are all mandatory. Evidence of performance must be collected regularly and used to inform decisions not filed away until the next external audit.
Clause 10: Improvement: When something goes wrong, there must be a documented process for addressing it, understanding why it happened, and preventing recurrence. Corrective action is not optional. It is the engine of continuous improvement.
Why This Matters for Health and Social Care Specifically
ISO 9001 is sector-neutral by design, but its principles align closely with what CQC, NHS commissioners, and local authorities already expect from quality providers.

The well-led domain of the CQC's assessment framework expects clear governance, accountability, and evidence of learning from incidents. That is Clauses 5, 9, and 10. The effective domain expects care that is evidence-based and outcome-focused. That is the process approach and evidence-based decision making. The responsive domain expects services organised around individual needs. That is customer focus and relationship management.
ISO 9001 does not replace regulatory compliance. But organisations that implement it well find that compliance becomes more manageable because the systems are already doing the work.
The Takeaway
ISO 9001:2015 is a serious standard. It demands genuine leadership commitment, functioning processes, documented evidence, and a real culture of improvement. Organisations that implement it well go beyond the requirements on paper they build something that genuinely changes how quality is managed day to day, and how consistently high standards are maintained under scrutiny.
Over the coming weeks I will be sharing reflections on each of the 10 clauses in more detail what they require, where organisations commonly fall short, and what good practice actually looks like.
Follow along if quality assurance, audit leadership, and regulatory compliance are relevant to your work.